The Emergency Aeromedical Service
The Emergency Aero-medical Service (EAS) commenced operations on the 4th June 2012, this pilot project was designed to evaluate the efficacy of a Helicopter Emergency Medical Service (HEMS) for Ireland. The Minister for Health, Dr James Reilly, accepted the findings of the project and has confirmed the clinical need for such a service in Ireland. The process is now underway to establish how best to provide a permanent dedicated service that will continue to serve the public and potentially expand to include an all-Ireland approach. Through this article we will reflect on the lessons learned by the crews working in this new environment, the introduction of new working systems and statistical analysis of the calls to date. The call sign for the helicopter is MEDEVAC 112.
The primary phase in developing the role of the EAS was on the operational development and complex infrastructure required to deliver such a service, Including the development of a dedicated National Aero-medical Co-ordination Centre (NACC) that co-ordinates all aero-medical calls including the EAS the Coast Guard and Air Ambulance transports. The training of the selected Advanced Paramedics focused teamwork with the Air Corps crewman and pilots and general orientation on safely operating together in this new environment. As the service developed a Clinical Governance framework has been introduced to ensure future development of EAS clinical operations remains patient focused and promotes a culture of continuous quality improvement.
At the heart of the EAS is an aspiration for clinical and operational excellence, uniformity of clinical practice and sound underpinning governance. The Clinical Governance Framework aims to provide a structure through which the EAS can deliver a high and consistent standard of clinical care and deliver a world class service for patients. The lessons learned in relation to communication skills, debriefing calls and using clinical governance meetings to share knowledge and improve standards can be replicated in ambulance bases throughout the country and in the wider health service.
Crew Resource Management (CRM)
Crew Resource Management (CRM) encompass expertise, experience and research from the aviation industry to improve the safety and efficiency of organizations involved in risky work. The introduction and application of CRM significantly changed the way in which National Ambulance Service (NAS) staff who work on MEDEVAC 112 have approached day to day practice.
CRM teaches us about human limitations and involves participants in assessments of their own behaviour and the behaviour of peers, it encompasses a wide range of knowledge, skills and attitudes including communications, situational awareness (SA), dynamic problem solving, decision-making, and overall teamwork. Additionally, participants in CRM training learn to understand how cognitive errors occur and are how external stressors such as fatigue, crisis management and work overload can contribute to human error.
Internationally these principles of managing the “Human Factors” have been successfully transferred into health services particularly in emergency care, surgery and anaesthetics CRM is now an essential part of air ambulance operations all over the world.
Below are just a few examples of how the principles of CRM and strong clinical governance can be incorporated into the wider arena of prehospital care.
Communication Skills
Clear communication can be something we take for granted during our day to day work at the side of the road at an RTC or working a cardiac arrest in a patients home but if you imagine running those calls in a noisy environment using a headset and radio suddenly you realize the importance of clear concise communication with your team the patient and family members. The restrictions placed on the helicopter crews by operating in this environment on a day to day basis makes you appreciate how simple clear communications can assuage a patients fear of the unknown, it can reduce stress on your team and it can alleviate errors. Our ability to communicate clearly while managing an emergency is a skill in its own right and should not be underestimated and is a skill that should be developed at every opportunity.
Situational Awareness
Having good Situational Awareness (SA) is a vital skill for helicopter pilots, and aircrews. It involves awareness of what is happening within the vicinity of the aircraft and the environment in which it’s operating, in order to understand how actions of team members may impact future goals and objectives. Advanced Paramedics assigned to EAS have developed a newly found appreciation for SA, not just in relation to aviation safety, but also having to make decisions about which hospital the patient should be brought to and the factors that may influence that decision. This involves considering the patient’s clinical condition and age, along with the capability of the receiving hospitals to manage specific illness or injury, the weather condition, access to helipads, etc. The challenge is using all this information to ensure the “right patient” is brought to the “right hospital” on each call, and utilising the speed and range of the AW139 helicopter to best advantage. Reconfiguration of regional hospitals into grouped trusts, along with the centralization of major Trauma, Cardiac and Stroke centres will continue to challenge all prehospital practitioners while making these decisions.
Consider you own region and your patient’s needs allowing with early appropriate decisions about the most appropriate means of transport, particularly in cases where time-sensitive interventions may be required
Challenge Response Checklists
In any emergency, there is a lot of multitasking going on, both by individuals and teams of responders. Understanding the limitations of the human brain in these stressful environments has led to the development of Challenge & Response Checklists. Originally a concept unique to aviation, they are used to ensure simple cognitive errors do not occur during pre- and post-flight checks and in the high stress environment of emergency situations. Pre-hospital emergency care has seen the development of similar checklists for use during the management of Cardiac Arrest, Return of Spontaneous Circulation (ROSC), Post Intubation Care, and the management of major haemorrhage.
Debriefing
After each call or at the end of the shift all the crew gather together to debrief the call. This process only takes on average 5 or 10 minutes but has repeatedly proven to be highly beneficial. During the debrief we take each aspect of the call from initial tasking to mission to handover at the receiving facility. This frank open discussion of each call with people taking ownership of both the positive elements and any errors that may have occurred, also highlighting how each aspect can be improved continual drives the service and each individual forward. We share our learning points in a simple feedback form which is left in the base for other crew members to learn from, we also close the loop of communication back to the National Aero-medical Co-ordination Centre (NACC) to ensure they also share in the learning/feedback process.
Clinical Governance Meetings

Each month we hold a clinical governance meeting, these meetings are attended by the on-call duty crew and at times other crew members will attend. The purpose of these is to exchange and share knowledge, highlight and address any operational or clinical issues, and promote future education and research. All with a view towards improving the quality of service to the wider NAS and the general public.
Each clinical governance meeting includes at least two of the following:
- Clinical cases review / presentation.
- Data Audit / Journal Review.
- Review of policies, procedures and guidelines.
- Training specific to EAS operations.
- Discussion of adverse events and critical incidents.
Teamwork and Feedback
Success of any aero-medical service depends on every member of the team, from strong medical and operational leadership to the National Aero-medical Co-ordination Centre (NACC) and the regional controls, the pilots, Advanced Paramedics and crewmen, the technical crews maintaining the aircraft and most importantly the frontline staff of the National Ambulance Service who been have been using the service to benefit their patients.
To date we have been able to measure and improve the teamwork and service to the NACC by closing the loop of communication and seeking feedback on cases attended.
In an effort to continually improve the service to the Patient, the prehospital practitioners caring for those patients and the wider health service, the crews of MEDEVAC 112 would greatly appreciate constructive feedback from NAS Practitioners as to their experiences with the EAS and how we can improve the service; with this in mind we have established an email link specifically to gather information about these interactions. Please feel free to email us on
eas@hse.ie
In your email please include your contact phone number PHECC pin and date of interaction or request for the EAS, please do not use any patient identifiers in your email. We will attempt to reply to your email in a timely fashion but as you can appreciate they will be managed by operational crews.
David Hennelly AP MSc
Clinical Development Manager
National Ambulance Service
EAS Statistical Analysis 04th June 2012 – 30th Nov 2013
Statistics courtesy of the Irish Air Corps
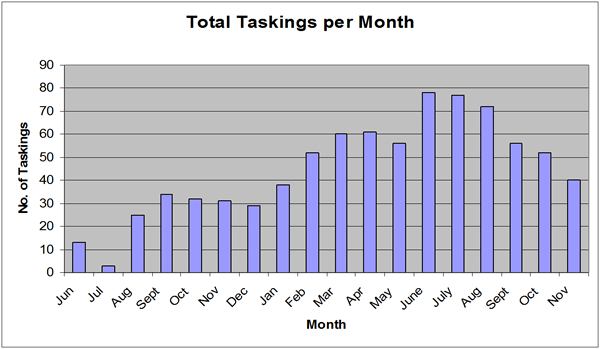
Tasking Frequency
Tasking Frequency maps the number of times MEDEVAC 112 has been tasked by the NACC, these figures will not represent the total number of aero-medical support requests by practitioners as requests may have been denied by the NACC prior to notification, or dealt with by the Coast Guard if MEDEVAC 112 was busy or unavailable. If aero-medical support is unavailable the NACC will endeavour to explain to the regional controls the rationale, all staff are encouraged to disseminate this feedback to ensure staff continue to use the service.
The EAS has proven to be an excellent asset for patients requiring rapid smooth transport to specialist centres, however both nationally and internationally aero-medical services are limited by strict criteria surrounding weather and hours of operation. Similar to any equivalent service for those reasons a certain number of calls may be denied. The decision to deny any call must be made by the NACC or the crew of MEDEVAC 112, regional control centres should inform the NACC of all requests from prehospital practitioners for aero-medical support and feedback as much information as possible to frontline crews to encourage continued use of this vital service.
The geographical distribution of tasking paints an interesting picture, as you can see the majority of calls are arising from the western and midland regions, naturally having the NACC based in Tullamore allows the NACC controllers to have a better insight into the calls that are occurring in their own region. The western region along with the Midlands has the option to simultaneously dispatch the EAS along with the local ground response, based on the information received from the caller. The recent centralisation of Cork/Kerry and Navan control into Townsend St, may allow further growth of the service in responding to calls in the southern and north eastern counties. The continued development of the service in these regions does depend on early appropriate activation by the crews on the ground and good awareness and initiative form the EMC’s in those regions. You can follow this link to get a better insight into the role of the EAS;
http://youtu.be/b-MPlILHHvk
Geographical distribution
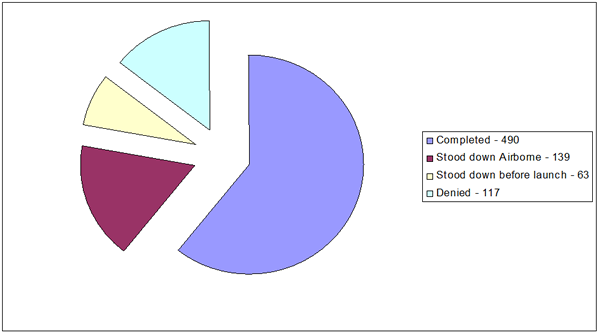
Receiving Hospitals and Call Classification
*Classification of calls are based on the number of calls completed
*161 STEMI cases are incorporated in ‘Medical’.
Increasingly, internationally peer-reviewed literature supports the survival benefit for patients treated in specialist centres following presentation with either serious illness or injury. These patients include those with severe trauma, as well as those who have suffered a stroke or a STEMI and who require time-sensitive interventions. The further National development of designated major trauma and PPCI centres will result in an increase in tertiary referrals, requiring both ground and air ambulance services to work closely to ensure that patients are taken to the most appropriate facility directly from the scene of accident or incident. EAS has proven that it can deliver a consistently high standard of clinical care, along with the ability to bypass closer, less appropriate centres, delivering the patient a level of service in-line with international best practice.